

After 40, your body’s hormonal landscape shifts in ways that can feel confusing and, frankly, alarming. Testosterone begins its slow decline, yet the effects of dihydrotestosterone (DHT) on sensitive tissues like the prostate can actually intensify. Understanding this dynamic isn’t just academic; it’s practical information that shapes how you respond to symptoms, when you seek medical care, and what questions you ask your doctor.
This guide explains the real relationship between DHT imbalance and prostate health, specifically through the lens of what changes after 40.
What DHT Actually Is and Why It Matters After 40
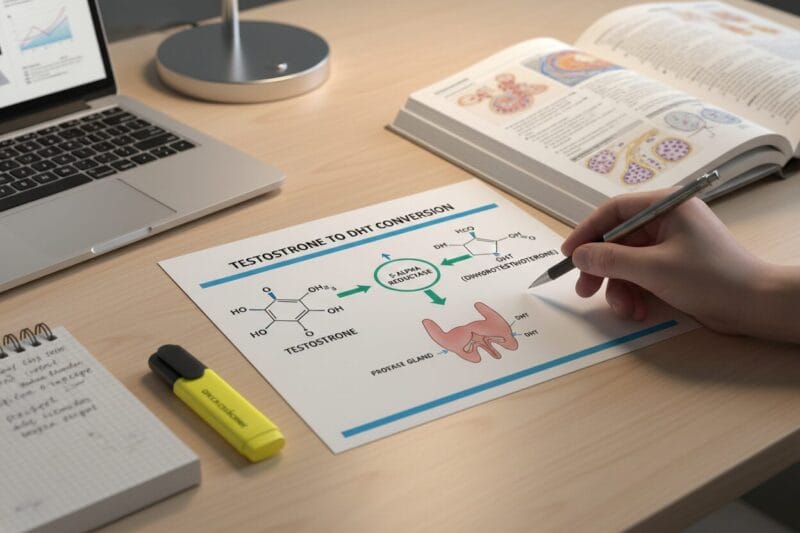
DHT, or dihydrotestosterone, is a hormone derived from testosterone through a conversion process driven by an enzyme called 5-alpha reductase (5-AR). Once converted, DHT binds to androgen receptors with roughly three to five times more potency than testosterone itself. That binding strength is what makes DHT so biologically significant, for better and for worse.
During puberty and early adulthood, DHT drives male development: facial hair, muscle density, genital maturation, and prostate growth. In the post-40 years, that same potency becomes a double-edged factor. Testosterone levels decline at roughly 1% per year after age 30, yet 5-alpha reductase activity doesn’t necessarily slow at the same rate, meaning DHT’s proportional influence can persist or even increase relative to testosterone.
Two types of 5-alpha reductase are relevant here. Type 1 is found primarily in the skin and liver, while Type 2 is concentrated in the prostate, hair follicles, and seminal vesicles. It’s the Type 2 enzyme that drives most of the prostate-related DHT activity men over 40 need to understand.
How DHT Accumulates in the Prostate
Here’s a detail most general articles skip over: your prostate doesn’t just receive DHT from the bloodstream. It produces its own. As the Cleveland Clinic explains, “Your prostate can produce large amounts of DHT. This local DHT production stimulates normal prostate growth.”
This intraprostatic DHT production is clinically critical because it means serum (blood) DHT levels don’t tell the whole story. A man can have DHT readings within a “normal” reference range on a lab test and still experience significant DHT-driven prostate changes, because the prostate’s local DHT environment can be far more concentrated than what circulates in the blood.
This also explains a common frustration: men who are told their hormone levels look fine but continue experiencing urinary or prostate symptoms. Understanding how DHT levels connect to prostate tissue changes is a necessary step before assuming bloodwork alone gives you the full picture.
DHT and Benign Prostatic Hyperplasia: The Core Connection
Benign prostatic hyperplasia, commonly called BPH, is a non-cancerous enlargement of the prostate gland. It’s one of the most prevalent conditions affecting men over 50, and its roots begin forming in the decade prior. DHT is the primary driver of the cellular proliferation that causes the prostate to grow beyond its normal walnut-sized dimensions.
BPH prevalence climbs steadily with age. Roughly 50% of men in their 50s show histological evidence of BPH, rising to over 80% by their 80s. As the prostate enlarges, it compresses the urethra, which runs directly through the gland, producing urinary symptoms that range from mildly inconvenient to significantly disruptive.
Common BPH symptoms include:
- Frequent urination, especially at night (nocturia)
- Weak or interrupted urine stream
- Difficulty starting urination despite urgency
- Feeling of incomplete bladder emptying
- Urinary tract infections due to retained urine
Clinicians often use the International Prostate Symptom Score (IPSS) to quantify severity, with scores above 20 classified as severe and typically triggering a conversation about active treatment. Research published in the Annals of Internal Medicine confirms that BPH increases with age and can substantially decrease quality of life for older men, reinforcing why early awareness matters.
The Hormonal Shift After 40: Both Directions of DHT Imbalance
Most discussions about DHT imbalance focus exclusively on excess. But the keyword here is imbalance, and that cuts both ways. Men over 40 can experience problems from DHT that’s too high and from DHT that’s fallen too low, particularly if they’ve pursued aggressive hormonal interventions or have underlying conditions.
Elevated DHT symptoms: Prostate enlargement and related urinary symptoms, accelerated male-pattern hair loss (androgenic alopecia), increased sebum production and acne, and potential worsening of existing prostate conditions.
Low DHT symptoms: Reduced libido and sexual dysfunction, depression and mood disturbances, decreased muscle mass and physical endurance, and exercise-induced leg cramps in older men.
That last point surprises many people. According to research summarized by PlexusDx, reduced DHT levels can result in depression symptoms, decreased sexual desire, exercise-induced leg cramps, and reduced muscle mass. Men who aggressively suppress DHT through medications or supplements without medical supervision may trade one set of problems for another.
The clinical goal isn’t to eliminate DHT. It’s to keep it within a functional range where it supports normal physiology without driving pathological tissue changes in the prostate.
DHT and Prostate Cancer: A More Nuanced Picture
One of the most anxiety-provoking questions men ask is whether elevated DHT increases their cancer risk. The honest answer is that the relationship is more complex than the popular narrative suggests.
The conventional assumption is straightforward: DHT stimulates prostate cell growth, therefore higher DHT means higher cancer risk. But peer-reviewed research complicates that model. A 2020 study published in PubMed found that DHT is negatively associated with long-term prostate cancer death regardless of clinical presentation, meaning higher DHT levels were associated with lower prostate cancer mortality, not higher.
This doesn’t mean DHT is protective in a clinically proven sense. What it does mean is that the biology is more nuanced than a linear “more DHT equals more cancer risk” framework. DHT clearly drives BPH, which is a structural, benign condition. Its relationship to prostate cancer risk and mortality is far less straightforward.
That said, regular PSA screening and urological checkups remain essential for men over 40, regardless of DHT levels.

Treatment Options: From Watchful Waiting to Medication
When DHT-related prostate symptoms become clinically significant, several treatment pathways exist. The right approach depends on symptom severity, prostate volume, patient age, and individual risk tolerance.
Watchful Waiting: Appropriate for men with mild IPSS scores (below 8) and no significant quality-of-life impact. Regular monitoring, annual PSA tests, and digital rectal exams form the core of this approach.
5-Alpha Reductase Inhibitors (5-ARIs): The primary pharmacological intervention for DHT-related BPH. Two drugs dominate this category:
- Finasteride (Proscar): Blocks Type 2 5-alpha reductase specifically, typically reducing prostate volume by 20 to 30% over 6 to 12 months of use.
- Dutasteride (Avodart): Blocks both Type 1 and Type 2 5-AR isoforms for more complete DHT suppression, often preferred for larger prostates or cases where finasteride shows insufficient response.
As Rezum’s clinical resource states, “By blocking DHT, 5-alpha reductase inhibitors can stall the growth of the prostate and eventually cause it to shrink,” which helps restore normal urinary flow. However, 5-ARIs carry real side effects: reduced libido, erectile dysfunction, decreased ejaculatory volume, and in some men, persistent sexual side effects that continue after discontinuation, sometimes called post-finasteride syndrome.
Men considering 5-ARIs should have an explicit conversation with their urologist about the benefit-to-risk profile relative to their specific symptom severity. These medications are not appropriate for mild BPH where lifestyle changes remain viable.
Lifestyle Factors That Influence DHT and Prostate Health
Pharmaceutical intervention isn’t the only lever available. Several lifestyle factors meaningfully influence DHT metabolism and prostate tissue health, with none of the side effect risks associated with medications.
Diet and Inflammation: Chronic low-grade inflammation amplifies DHT’s proliferative effects on prostate tissue. Diets high in processed foods and refined carbohydrates promote this inflammatory state, while Mediterranean-pattern diets rich in tomatoes (lycopene), cruciferous vegetables, fatty fish, and green tea have been associated with lower BPH risk in observational studies.
Body Composition: Visceral fat increases aromatase activity, converting testosterone to estrogen and shifting the androgen balance in ways that can worsen prostate tissue sensitivity. Maintaining a healthy weight reduces this hormonal interference.
Zinc: A natural inhibitor of 5-alpha reductase activity, zinc is found in higher concentrations in the prostate than in any other organ. Zinc deficiency has been associated with increased DHT activity, and dietary sources include oysters, pumpkin seeds, beef, and legumes.
Exercise: Regular moderate-intensity aerobic and resistance training supports healthy testosterone metabolism, reduces visceral fat, and lowers systemic inflammation. Sedentary behavior is independently associated with worse BPH outcomes.
Connecting the Dots: Hair Loss, DHT, and the Prostate
Harvard Medical School notes that male-pattern baldness and prostate disease are both androgen-driven conditions sharing DHT as a common biological driver. Men who experience significant androgenic alopecia before 40 are essentially observing their androgen receptor sensitivity in real time. High receptor sensitivity to DHT in hair follicles often correlates with similar sensitivity in prostate tissue.
This doesn’t mean hair loss guarantees prostate problems. But it does mean men with significant early hair loss have an additional reason to be proactive about prostate monitoring as they move through their 40s. Both conditions reflect the same underlying biology: androgen receptors responding robustly to DHT’s binding signal.
If you’re navigating multiple DHT-related symptoms and want a structured look at products designed to address this hormonal interplay, our comprehensive DHT and prostate supplement review covers the evidence behind leading formulations in this category.
When to See a Doctor
Knowing when to escalate from self-monitoring to professional evaluation is important. Several signals warrant prompt urological consultation:
- Any blood in urine or semen
- Sudden inability to urinate (acute urinary retention)
- IPSS score above 15, or symptoms worsening over months
- PSA levels rising year over year, even within the “normal” range
- Pain in the pelvic region, lower back, or during urination
Men over 40 should establish a baseline PSA test if they haven’t already. The value of a single PSA reading is limited; tracking PSA velocity over time is where the real diagnostic value lies. Rising PSA, even from a low baseline, can signal prostate changes that warrant investigation.
